
As originally published in the International Journal of Emergency Mental Health and Human Resilience, Vol. 16, No. 143-148, pp. ISSN 1522-4821
Treating Veteran Posttraumatic Stress Disorder Using the Comprehensive Resource Model
By Katherine A. Heeg
Abstract
The Comprehensive Resource Model is a groundbreaking psychotherapeutic treatment modality with broad possibilities for use with the military veteran population. Objective: This article describes a clinical case example where this modality was used with a veteran presenting with severe PTSD symptoms. Method: Six 60-75 minute treatment sessions are described. Symptoms were measured before and after treatment and at a two-year follow-up using the Posttraumatic Diagnostic Scale, Hospital Anxiety and Depression scale, and Clinical Global Impression scale. Results: Findings showed that the treatment was effective at relieving symptoms of dissociation and flashbacks, even after two years. Some symptoms remained such as hypersensitivity to loud noises. Conclusion: The Comprehensive Resource Model, specifically the Resource Energy Grid, provided a safe, effective way to treat some very challenging symptoms. Studies on larger sample sizes would be necessary for generalizability. An Appendix by the spouse of the subject provides additional support for the findings.
Keywords: Comprehensive Resource Model, combat PTSD, dissociation, Resource Energy Grid
The purpose of this article is to introduce the Comprehensive Resource Model of psychotherapy with a clinical case study. The Comprehensive Resource Model was formerly called the Resource Model of Brainspotting. To date, no articles or books have been written specifically about this model in the professional literature. This case report attempts to test the effectiveness of the Comprehensive Resource Model, specifically a clinical tool called the Resource Energy Grid. Pre and post-treatment questionnaires are used to measure results. This article attempts to show that the Comprehensive Resource Model is a practical and effective therapeutic modality for treating Posttraumatic Stress Disorder related to military service.
The Comprehensive Resource Model is a new psychotherapy treatment for Posttraumatic Stress Disorder (PTSD) and Complex Posttraumatic Stress Disorder. It has some similarities to the evidence-based treatment Eye Movement Desensitization Reprocessing (EMDR), and Brainspotting, a modality that uses focused eye position. While EMDR primarily uses eye movements, Brainspotting predominantly uses focused eye positions. Corrigan and Grand (2013) define Brainspotting:
Brainspotting is a psychotherapy based in the observation that the body activation experienced when describing a traumatic event has a resonating spot in the visual field. Holding the attention on that Brainspot allows processing of the traumatic event to flow until the body activation has cleared. This is facilitated by a therapist focused on the client and monitoring with attunement (p. 1). Grand (2010) further defines Brainspotting below.
A "Brainspot" is the eye position which is related to the energetic/emotional activation of a traumatic or emotionally charged issue within the brain. Located by eye position, paired with externally observed and internally experienced reflexive responses, a Brainspot is actually a physiological subsystem holding emotional experience in memory form. Brainspotting stimulates and promotes deep processing, integrating, and healing activity within the brain. This appears to take place within the brain’s emotional centers at a reflexive and cellular level. It typically results in a de-conditioning of previously conditioned, maladaptive emotional, psychological, and somatic responses and patterns. It appears to stimulate, focus, and activate the body’s inherent capacity to heal itself from trauma.
The Comprehensive Resource Model appears to take the above process even further. It adds six nested, primary therapy resource tools and four secondary resource therapy tools which are utilized sequentially, concurrently, or individually as needed throughout the therapy work. The use of these layered resources creates a streamlined, highly effective level of somatic resourcing and neurobiological rewiring (Schwarz 2009). The component of the Comprehensive Resource Model which was used as the primary tool in this particular case is called the Resource Energy Grid, during which a client identifies grounded, centered, present, or solid areas of the body and connects them together, creating an internal resource, and from there, a corresponding eye position is found which anchors this state physiologically, and the traumatic reprocessing work begins. Lisa Schwarz, MEd., developed the Comprehensive Resource Model (Schwarz 2009). Brainspotting was used in her clinical psychology practice with clients diagnosed with Dissociative Identity Disorder (DID) and Dissociative Identity Disorder Not Otherwise Specified (DDNOS), and the Comprehensive Resource Model evolved out of her work with that population (Schwarz 2009). The first research study on Brainspotting has been completed (Grand, Hildebrand, & Stemmler, in press). An upcoming book The Comprehensive Resource Model for the treatment of complex posttraumatic stress disorder is currently being written by Frank Corrigan and Lisa Schwarz (L. Schwarz, personal communication, January 13, 2014).
Working with Trauma and Dissociation
In the DSM 5 diagnostic criteria for Posttraumatic Stress Disorder, exposure to actual or threatened death through directly experiencing the traumatic event is one way the disorder might develop. Dissociative symptoms are considered “intrusion symptoms associated with the traumatic event(s), beginning after the traumatic event(s) occurred” (DSM 5, 2013, p. 271). Recurrent distressing memories and dreams related to trauma may occur, or:
Dissociative reactions (e.g., flashbacks) in which the individual feels or acts as if the traumatic event(s) were recurring. (Such reactions may occur on a continuum, with the most extreme expression being a complete loss of awareness of present surroundings.) (DSM 5, 2013, p. 271).
Robert Scaer (2004) coined the term “trauma capsule” to describe traumatic memories held in the brain. The Comprehensive Resource Model attempts to resolve the problem of trauma capsules. Scaer best describes dissociation within PTSD below.
Dissociation has its roots in the procedural memories for remote traumatic events, and that the confusion between past and current events is the defining feature of dissociation. Current thinking would suggest that when patients have dissociated, they are experiencing distorted perceptions in a variety of possible areas – reality, time, memory, sense of self, sense of the body, etc. In fact, what they are experiencing are perceptions that have been stored in survival-based procedural memory as if they reflect the experience of the present moment. . . The primary diagnostic criteria for PTSD reflect that posttraumatic symptoms to a significant degree relate to abnormal memory processes – dreams, flashbacks, intrusive thoughts and images, cue-related anxiety and startle, avoidance of exposure to reminders of the trauma. Although the other important criteria for PTSD include arousal and avoidance criteria, one could make the case that the entire symptom complex of PTSD is based on the premise that an event that occurred in the past is perceived as a lived event that is still in the present. . . .trauma therefore could be defined as a corruption of perception of time and memory. . . .The primary function of procedural memory is the acquisition of information and skills that are necessary for survival. And most of these have to do with the unconscious functioning of your body (pp. 2-3).
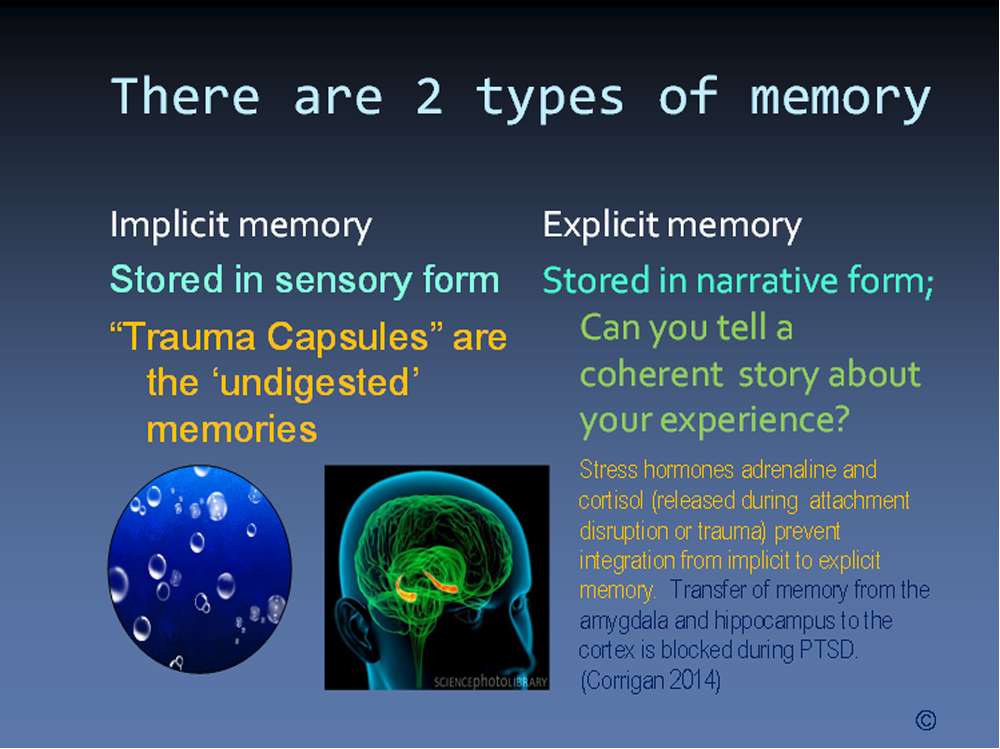
Furthermore, implicit memories are stored in sensory form, while explicit memories are stored in narrative form. Stress hormones adrenaline and cortisol (released during attachment disruption or trauma) shut down the hippocampus, preventing integration from implicit to explicit memory (Image 1). In Image 1, the circle containing bubbles represents the trauma capsules, or disturbing life experiences we accumulate over time. The way we make a memory is similar to the way we digest food: our bodies take what we need for nourishment and eliminate the waste. In order for a memory to “digest,” it must process through the hippocampus, which is shown in the bottom center of Image 1. When a traumatic event is experienced, stress hormones adrenaline and cortisol are released, stopping the memory from being integrated into explicit memory, and the memory remains stuck in its sensory state form (Schwarz, 2009). For example, if one was asked “What did you have for breakfast three weeks ago today?” The majority of us will not be able to recall that information. However, if what was consumed for breakfast three weeks ago made the individual violently ill and required a trip to the emergency room, the individual would most likely remember what was eaten because this information caused the trauma of becoming sick, and is then necessary to retain for survival. With Comprehensive Resource Model therapy, traumatic memories are accessed through either eye position or body activation and process through the hippocampus, releasing the disturbing aspects of the traumatic memory until it is no longer bothersome and can integrate into autobiographical memory.
Image 1
A New Model
One of the biggest challenges in treating the mental health symptom of dissociation during trauma treatment is keeping clients grounded and supported while reprocessing disturbing life experiences or traumatic memories without becoming emotionally flooded, detached, ungrounded and “checked out” or dissociative. While other trauma therapies might suggest in their theoretical conceptualization that a client presenting with dissociative features “is not ready” for trauma reprocessing work, the Comprehensive Resource Model provides a safe, effective way to help clients reprocess traumatic memories. The Resource Energy Grid is a clinical tool that works like this: the therapist asks the client to direct his or her attention inward to the body and find a physical location that feels grounded, centered, solid, or present; the client says “my feet feel okay;” then the therapist asks the client to identify another grounded, centered, solid, or present spot, and the client says “my knees” and the therapist instructs the client to draw an imaginary line on the inside of the body connecting the feet up to the knees. In this manner, a series of seven “okay” spots, including a distress release spot, are linked together. This works even within people who often have multiple somatic complaints. From there, the therapist assists the client in finding the eye position that corresponds with the felt sense of the connected points, or the grid as a whole. The client is invited to stay on this eye position while the trauma material is remembered, released, and re-processed (Schwarz 2009). Comprehensive Resource Model clinicians have found that by using this Resource Energy Grid as a tool, dissociative clients manage to stay present during therapeutic work and the majority do not decompensate after sessions or between sessions during which they reprocessed deeply disturbing traumatic life experiences. For clients who are unable to “find” any felt sense of somatic resources as building material for this tool, the use of other components of the Comprehensive Resource Model are mobilized in order to allow for somatically dissociated clients to achieve success in terms of developing a conscious connection to their body (Schwarz 2009).
The Comprehensive Resource Model has clients evaluate their own distress levels. This is accomplished through the Subjective Units of Disturbance scale (SUD), which was created by Joseph Wolpe (1969). This scale is used by therapists to evaluate client distress levels and indicate client progression. Clients are asked, “On a scale of zero to ten, with ten being the worst distress level imaginable and zero being no bother or neutral, how much does the traumatic incident bother you now?” During EMDR treatment, the goal is to achieve a zero SUD score. Unlike EMDR, Comprehensive Resource Model clinicians might instruct the client to increase their SUD score as high as it will go by saying, “Close your eyes and go inside and think of the traumatic event and do whatever you have to do to activate the distress level as high as it will go.” In the context of this high level of distress, when neurobiological resources are identified and developed before the actual processing begins, the power and effectiveness of the resourcing throughout the trauma work is assured (Schwarz 2009). It appears that reactivating the psychological distress level aids in accessing and processing out or extinguishing the remaining emotional, physiological, and somatic activation. Repetition is required for learning any new behavior, and it seems that by repeating this process, the new, more adaptive neuropathways become strengthened.
Single-Subject Design
Single-subject designs have played an important role in the history of behavioral research. Reading an individual case study can be more tangible than abstract data from a larger study. Rubin and Babbie (1993) write:
Significant scientific advances do not necessarily require the use of large-scale studies that attempt to verify hypotheses. Important contributions also can be made by exploratory studies that use more flexible methods, including smaller samples, in efforts to discover new insights and generate hypotheses and theories for which generalizability can be tested later in more tightly controlled studies using larger, probability samples (p. 297).
Pre-treatment, post-treatment, and follow-up assessments were administered by the author. The assessment instruments used were: The Posttraumatic Diagnostic Scale (PDS; Foa, 1995); the Hospital Anxiety and Depression Scale (HADS; Zigmod & Snaith, 1983); and the Clinical Global Impression (CGI), which is used to assess treatment response in psychiatric patients. The questionnaires were given prior to the first session, at the fifth session, and two years following the conclusion of treatment.
The Posttraumatic Diagnostic Scale, or PDS, is described below by Foa, E., Cashman, L., Jaycox, L., & Perry, K. (1997).
The PDS is a 49-item self-report measure recommended for use in clinical or research settings to measure severity of PTSD symptoms related to a single identified traumatic event. The PDS has four sections. Part 1 is a trauma checklist. In Part 2, respondents are asked to describe their most upsetting traumatic events. . . Part 3 assesses the 17 PTSD symptoms. Respondents are asked to rate the severity of the symptom from 0 ("not at all or only one time") to 3 ("5 or more times a week / almost always"). Part 4 assesses interference of the symptoms. The PDS yields a total severity score (ranging from 0 to 51).
The PDS has been validated on individuals aged 18-65 (Foa, 1995). Results were hand scored by the author.
The Hospital Anxiety and Depression Scale (HADS) was developed by Zigmond and Snaith (1983) and is commonly used by doctors to determine the levels of anxiety and depression that a patient is experiencing not related to medical illness. The HADS is a 14 item scale; seven of the items relate to Anxiety (A) and seven relate to Depression (D). There are three categories for scoring the HADS: 0-7 = Normal, 8-10 = Borderline abnormal (borderline case), and 11-21 = Abnormal (case).
The Clinical Global Impressions scale (CGI) is a three-item observer-rated scale commonly used to measure symptom severity, global improvement, and therapeutic response. For this case study, only one of the three items was used, the CGI Improvement scale. This is a seven point scale that requires the clinician to assess how much the patient's illness has improved or worsened relative to a baseline state at the beginning of the intervention and rated as: 1-significantly improved; 2-much improved; 3-minimally improved; 4-no change; 5-minimally worse; 6-moderately worse; or 7-significantly worse.
Case Report
Mark was a 29 year-old biracial married man who came to treatment after a disturbing dissociative episode. Mark served in the military for eight years; five years included active duty combat deployment overseas. Mark served in a leadership position and received an honorable discharge. While deployed, Mark escaped some life threatening situations, but what was most difficult for him was assigning which of his fellow soldiers went out on convoys. One of his comrades “didn’t make it back” and another one lost his legs.
Mark reported that when he went through his exit process from the Marines, he was evaluated by a psychiatrist. When the psychiatrist told him he had PTSD, he dropped out and refused to return to her or any other military service related mental health evaluator. He reported his reason was that he did not want to be “drugged up” (prescribed large amounts of psychotropic medication). Mark was accurate here; Bessel van der Kolk (2007) states that “A good psychological intervention like eye movement desensitization and reprocessing (EMDR) has an effect size of 2.2 compared with an SSRI having an effect size of 0.48. It is about 5 times as powerful.” Mark acknowledged having a tough time re-entering the civilian world, and frequently found himself engaging in physical altercations. Mark also reported jumping out of moving vehicles, including one occasion when he jumped out of a car and disappeared into the woods. Alcohol was not a factor in that incident; he appeared to be in a dissociative state at the time. He also reported taking his anger out on himself and objects, such as punching a cement cinder block which left him with a broken arm. This information was provided at the first interview, when the PTSD diagnosis was confirmed by the author. Prior to his military service, Mark did not have rage attacks, dissociative episodes, nightmares, or flashbacks.
Presenting Problem
The dissociative rage incident that precipitated Mark’s entry into treatment happened when Mark went to watch a sibling graduate from the same training camp he went through. His wife Rhonda reported that he appeared “glazed over” during the graduation ceremony. Then Mark went out to celebrate with his sibling at a bar. Mark reports having a few drinks, then ending up in a fight with five other men, during which he ripped the toilet seat lid off the toilet from the bar bathroom and was using it as a bat to attack. By the time he got back to his hotel room, the clerk at the hotel called the police on Mark and was visibly afraid of him. Mark proceeded to go to his hotel room and began shouting military commands at his wife to take cover under the bed to avoid incoming fire. To Rhonda, it was clear that Mark was having another dissociative rage attack.
Other clinically significant symptoms that meet criteria for a Posttraumatic Stress Disorder diagnosis included occasional flashbacks, nightmares about the flashbacks, triggers such as lights and sirens from ambulances, and fireworks exploding. Certain vibrations would also cause a startle response, and movies like the film “Jarhead” about the psychological endurance test of being at war in a desert elicited helpless feelings. Mark stated that he was unable to finish watching that film. Mark also reported poor concentration and inability to focus. Mark said that when he tried to concentrate, he felt overwhelmed and could not focus. At the time of treatment, he was working on completing his Bachelor’s degree while also working full time in his family business.
Course of Treatment
Mark was seen a total of six sessions. Mark’s wife Rhonda sat in on the first session and provided her perspective on Mark’s personal history. This was helpful since she knew him prior to his deployment. Sessions two, three, and four were Comprehensive Resource Model sessions lasting 60 minutes; one session lasted 75 minutes. Sessions five and six are also described, and a two year follow-up interview was conducted via video conference.
Sessions One & Two
The first session consisted of completing the pre-test questionnaires, history taking, and introduction to Comprehensive Resource Model by experiencing a partial Resource Energy Grid. Mark responded well, and appeared to understand the benefit of what was happening. He reported feeling less anxiety, even with only five to ten minutes on his Resource Grid eye position. During the second session, a complete Resource Energy Grid was used and paired with the corresponding eye position. From there, Mark reprocessed the worst experience of his time in the military. While en route to his destination, Mark was in a foreign developing country and he went out with his comrades who became intoxicated. The group attracted the attention of some organized crime members who, it appeared, were determined to make sure these soldiers did not make it home. Mark felt certain they would all be executed and appeared to have good reason to believe this. The experience lasted an entire night. During his reprocessing, Mark reported feeling many sensations in his brain. At one point he stated “It feels like someone is touching behind my eyes.” He reprocessed these events and by the end of the session reported his level of distress as neutral on the Subjective Units of Disturbance (SUD) scale. At the following session, Mark reported zero SUD level of disturbance for this incident, and he also reported feeling really good after the first session.
Session Three
At times, the Comprehensive Resource Model clinician must decide which tools to use during the session, such as whether or not to use a Resource Energy Grid or use a different tool. During the third session, the eye position where Mark felt the least distress was used for processing. Mark worked on memories that became triggered when he attended his sibling’s boot camp graduation. Seeing his brother’s accommodations brought his own experiences back which he described as difficult and overwhelming. Being picked on by an older soldier until he finally stood up for himself, along with some physically threatening moments administered by his drill sergeant, and a humiliating moment on the shooting range made Mark feel jittery in his heart with SUD level of six or seven. Reprocessing was done and SUD level went to zero. In this instance, a Resource Energy Grid was not used because Mark was already significantly activated; to stop and build a grid might have interrupted his process. This author/clinician thought Mark would be able to process adequately without it for this session and indeed that turned out to be the result. This is an issue of using one’s experience and clinical judgment. This develops from client attunement, observation, and the clinician’s best educated guess as to the outcome of applying a particular intervention.
Session Four
For his fourth session, Mark wanted to reprocess a memory which he had previously reported was his second worst life experience. A Resource Energy Grid was used for this session. This incident happened after returning from deployment. Mark’s father experienced a life threatening injury (severe burns) while working in the family business. Mark had to take him to the hospital where he was placed in the Intensive Care Unit. SUD level was ten and Mark felt distressed in his chest and throat. Mark reported he had nightmares and flashbacks on the night of the incident. Mark successfully reprocessed his shock, sadness, and feelings of helplessness. He reported feeling neutral at the end, with SUD of zero.
Session Five
At the fifth session, Mark completed his post treatment questionnaire. He reported he was feeling so good that he cancelled his psychiatric evaluation which he had scheduled after his dissociative incident. One disturbing memory remained that Mark wanted to work on. An RPG (rocket propelled grenade) exploded twenty-five feet from him. In the desert, the enemy used water, and when it evaporated, the RPG’s would detonate. Because Mark’s eyes kept returning to the same spot while recalling this event, this “activation” eye position was used as an anchor from which to do the processing work. It may have been the same direction he was oriented towards at the moment of explosion. In similar work with police and military, it appears there is sometimes a correlation between where the client is looking at the time of physical or psychological injury and the eye position that unlocks trauma reprocessing. Often, where the individual was looking at the moment of incident becomes the eye position essential for healing. Mark reprocessed this incident with incredible detail, recalling second by second what happened and how he felt physically, emotionally, and intellectually. At the end of his reprocessing, he was asked to bring up the image and said “it feels separate, detached.” Mark left the service with permanent partial hearing loss in one hear (most likely from this incident). Mark stated that these explosions were so commonplace, he did not even report it.
Session Six
At the sixth and final session, Mark reported no distress when he brought up the thought of RPG’s, explosions, or his time in the service. He discussed a tumultuous romantic relationship while in the service with another service member, but felt that he had successfully worked through those issues on his own as evidenced by his ability to completely trust his wife Rhonda. He reported that the Comprehensive Resource Model sessions had the effect of resetting his stress threshold. “Little things used to make me nuts and stress me out to the point that I can’t sleep or work and then I’d drink in excess.” Mark stated that he felt he returned to his pre-deployment personality. He added that prior to this treatment, he drank between three to six beers each night on weekdays, and could consume either an entire bottle of hard liquor (whiskey) on weekend nights, or three bottles of wine. He stated he stopped all on his own, and his last drink was three beers the previous weekend while at a wedding, but prior to that he consumed no alcohol for two weeks. In hindsight, it appears he was self-medicating his PTSD symptoms. Substance abuse becomes a common coping skill for many veterans with untreated PTSD. Mark appeared to be a reliable self-reporter; it seemed he self-disclosed this information because he was amazed by his own transformation.
Results
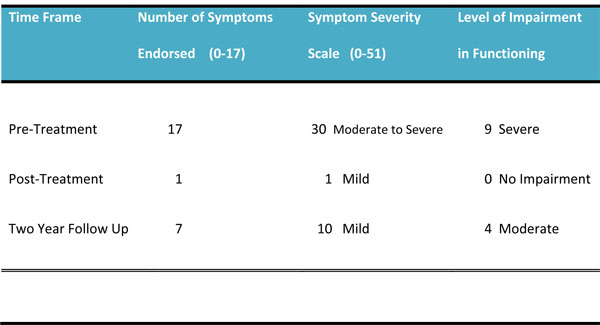
The PDS measures re-experiencing symptoms, avoidance symptoms, arousal symptoms, and level of impairment in functioning. The number of self-reported PTSD symptoms decreased immediately after treatment, followed by a small increase of symptoms at the two year follow up assessment (Table 1).
Posttraumatic Stress Diagnostic Scale (PDS) Results Table 1
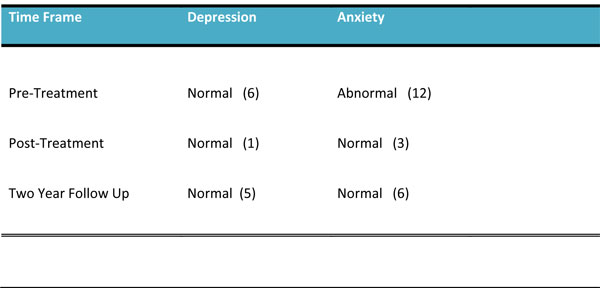
Mark’s HADS scores are shown below. There was a definite decrease from pre to post-treatment, however, while still in the Normal range, the two-year follow-up scores display some increase from the Post-Treatment scores, especially in the anxiety category (Table 2).
Hospital Anxiety and Depression Scale (HADS) Results Table 2
Regarding the CGI improvement scale, at the time of the post-treatment questionnaire, the clinician/author rated Mark as 1-significantly improved. At the time of the two year follow up clinical interview, the clinician/author again rated Mark as 1-significantly improved.
Discussion
During the two-year follow-up clinical interview, Mark reported that he had not had any nightmares, flashbacks, rage attacks, or dissociative episodes in the two years since his treatment. Mark stated that he does think about his military service frequently because he lives in a community with a high population of military personnel. He moved his family business to a new area due to lower cost of commercial real estate. When exploring the questionnaire answers during the two-year follow-up interview, Mark was asked why he felt slowed down or unable to concentrate. He replied that his baby just began sleeping through the night, and he has not been to the gym to exercise in a year. He said he felt “overwhelmed with things—probably from taking on too much.” Mark elaborated that all of his current stressors have to do with his work running a small family business in which the following responsibilities fall on him: customer service, sales, operations, developing new products, repairing machinery, and completing building renovations. Mark said the only PTSD related symptom that remained is his reaction to fireworks, which happen daily where he lives, even on a Tuesday evening in February. Mark explained that when he can see the fireworks he is fine, but when he cannot see them, his heart rate elevates. The elevated heart rate happens an average of once per week, since residents of Mark’s neighborhood enjoy fireworks year round. He stated for the most part he has gotten used to it and he appeared to be enjoying life in his new community. Appendix A shows post-treatment follow-up commentary from Mark’s wife Rhonda, which provides additional information and perspective on Mark’s functioning.
Mark’s hyperarousal to fireworks epitomizes Robert Scaer’s claim that procedural memories encode information and skills necessary for survival. For soldiers in theater, explosive noises can mean death, and even though Mark is consciously aware that fireworks happening nearby are not life threatening, his heart rate still elevates. Mark might benefit from some addition sessions with the goal of decreasing hypersensitivity to explosive noises.
Conclusion
The Comprehensive Resource Model is an effective way to treat combat PTSD, even in complicated cases with severe dissociation like Mark presented with. The small increase in symptoms measured by the assessment tools PDS and HADS appear to be from family and work related stressors, not prior PTSD symptoms, with the exception of loud noises described above. One benefit of the single subject design model is that the researcher can review answers with the subject in detail and ask “What was on your mind when you checked that answer?” and gather more relevant information that might not be obtainable with a larger sample size. However, n=1 is an extremely limited sample size. Could there be other reasons why Mark’s symptoms appeared to be eliminated? Due to the severity and persistence of his dissociative episodes and PTSD symptoms, it is unlikely that they stopped on their own, due to extinction or the passing of time. In the author’s experience, the Resource Energy Grid is an essential clinical tool. Without it, the clinician can unintentionally trigger a client’s trauma capsule holding psychological pain. Clients can become emotionally flooded and decompensate--the clinician’s equivalent to stepping on a landmine. Often, that leads current and former military service members to drop out of treatment, and give up on mental health services. The Resource Energy Grid provides an added safety feature: consider it the seatbelt for trauma work. Therefore, the Comprehensive Resource Model should be further explored by other clinicians and researchers looking to solve the problem of complex PTSD, especially when dissociative symptoms are present.
References
Clinical Global Impressions (CGI) Scale http://www.psychiatrictimes.com/clinical- scales-clinical-global-impressions-scale-cgi/clinical-scales-clinical-global-impressions-scale-cgi/clinical-global-impressions-scale-cgi
Corrigan F, Grand D. (2013). Brainspotting: Recruiting the midbrain for accessing and healing sensorimotor memories of traumatic activation [Abstract]. Medical Hypotheses, 10, 759-766. http://dx.doi.org/10.1016/j.mehy.2013.03.005
Diagnostic and Statistical Manual of Mental Disorders, 5th Edition: DSM 5. (2013). American Psychiatric Association. pp. 271-280.
Foa, E. (1995). Posttraumatic stress diagnostic scale manual. Minneapolis, MN: NCS Pearson, Inc.
Foa, E., Cashman, L., Jaycox, L., & Perry, K. (1997).
http://www.ptsd.va.gov/professional/assessment/adult-sr/pds.asp
Grand D. (2010). Retrieved from https://brainspotting.pro/ Retrieved in 2010.
Grand D. (2013). Brainspotting: The revolutionary new therapy for rapid and effective change. Boulder, CO: Sounds True.
Grand D, Hildebrand A, Stemmler M. (in press). A preliminary study of the efficacy of Brainspotting – a new therapy approach for the treatment of posttraumatic stress disorder.;Journal for Psychotraumatology, Psychotherapy Science and Psychological Medicine. Retrieved from the author.
Hospital Anxiety and Depression Scale rating scale scoring sheet retrieved from:
http://www.scalesandmeasures.net/files/files/Hospital%20Anxiety%20and%20Depression%20Scale%20(1983).pdf
Grand D. (2013). Rubin A, Babbie E. (1993). Research methods for social work. Pacific Grove, CA: Wadsworth, Inc.
Scaer, R. (2006). The dissociation capsule. http://www.traumasoma.com
Schwarz, L. (2009).The Comprehensive Resource Model for the treatment of complex PTSD: Training manual. Retrieved from the author.
Van der Kolk, B. (2007).http://www.traumacenter.org/resources/bvdk_interview.php
Appendix A
Post-Treatment Client Commentary from Rhonda
[Please note that the author had no communication with Rhonda from the time after the first appointment until the two year follow up. Mark’s wife, Rhonda, shares her perspective and experiences below.]
My thoughts on my husband’s treatment- Studying behavioral health, psychology, and being an LCSW still didn't prepare me to watch my husband suffering from the symptoms of PTSD. I knew what he was going through but felt so limited.
I knew that traditional talk therapy was the last thing my husband would participate in and in his desperation he agreed to a psychiatrist- I had my fears as I didn't want to just medicate the problem, I wanted him to process and gain a better understanding of what he was going through. Speaking with a colleague who was trained in EMDR, (a therapy I had success with personally) she recommended/referred me to you. My husband was open to going as it wasn't "talk therapy". I remember praying for some relief for him.
I sat in the first session and heard him share about experiences that he never spoke about; it took everything to hold myself back from tears. I remember him telling me he felt like his brain was moving, like an itch inside the brain. After his first session he slept through the night- no nightmares.
He continued to go and I was shocked at the changes; and over 2 years later I can say that those changes have stayed. No nightmares, drinks socially and not in excess (and even social drinking is rare) has had no dissociative episodes, can talk about his combat experience, and overall is less anxious. These changes have allowed him to live- we moved to North Carolina, bought a house and have an 8 month old son. We were able to go through his old Marine gear and memorabilia and packed it away to show our son one day- this was not even an option in prior years, it sat in the same bag since he left the corps never to be opened. It was something I always thought about- hoping he would look at his Marine memories and feel pride. I think he now can have that. I also have noticed that Mark makes eye contact now- he never looked people in the eye, rarely me. He has improved so much with this area it has helped him be a better [at work] and feel confident.
Of course his experience still plays a role in his life; he still chooses not to watch certain war movies and I notice mild anxiety with fireworks or loud noises such as a car backfiring. What once would cause him to shake and glass over now just gives him mild discomfort and he expresses it- usually acknowledging it is enough to decrease his anxiety to a 0.